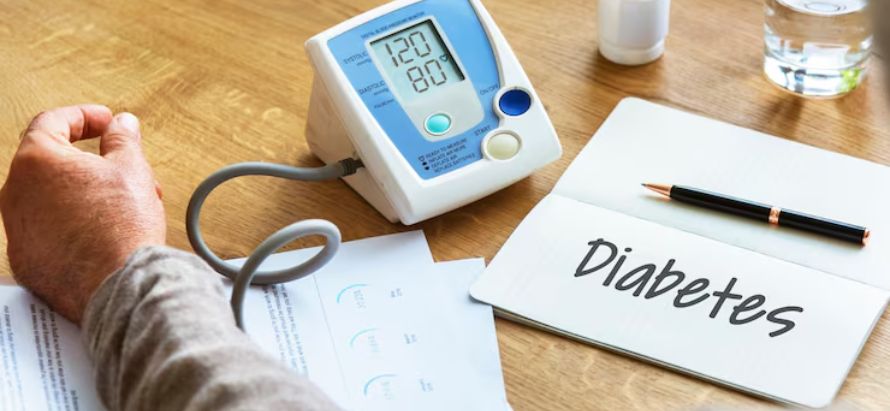
In a surprising shift, UnitedHealthcare, one of the largest U.S. insurers, announced a significant rollback of coverage for remote patient monitoring (RPM) services beginning January 1, 2026. Under the new policy, RPM will only be reimbursed when used for patients diagnosed with chronic heart failure or hypertensive disorders during pregnancy. Conditions such as type 2 diabetes and standard hypertension will no longer qualify for coverage.
The policy update was quietly published in September 2025 and affects commercial, Medicare Advantage and Medicaid plans operated by UnitedHealthcare. The company’s rationale: the current evidence base does not conclusively support RPM for many chronic conditions outside the two allowed categories. “Remote physiologic monitoring is not reasonable and necessary due to insufficient evidence of efficacy,” the policy document states.
Industry experts and providers have expressed concern. They point out that numerous studies show RPM’s benefit in managing hypertension and diabetes reducing hospital admissions and improving control of blood pressure and glucose levels. Critics argue that UnitedHealthcare’s decision may set a precedent for broader reductions in coverage of value-based digital health services, impacting millions of patients who rely on RPM to support chronic disease management.
UnitedHealthcare, meanwhile, emphasised that home-monitoring devices may still be covered under member benefit plans, but the time clinicians spend monitoring and acting on transmitted data outside the two approved conditions will not be reimbursed. The shift will force many providers and patients enrolled in RPM programmes to re-evaluate protocols, potentially discontinuing monitoring services for diabetes and hypertension.
As the 2026 implementation date approaches, the move raises several questions: how this aligns with Medicare policy, whether quality of care will suffer, and whether patients will be left with fewer options for proactive, home-based disease management. The change underscores the uncertain future of RPM reimbursement even as digital health tools continue to grow in adoption and complexity.